Stress Incontinence
Below is a clinically oriented, anatomy-to-function explanation of the ligaments and connective tissue systems that maintain the normal position of the female urethra, their relationship to the bladder base, and how their failure leads to stress urinary incontinence (SUI).
Normal anatomical relationships Bladder-urethra unit
• The female urethra (::::3-4 cm) is not an isolated tube; it functions as part of a
bladder-urethral unit.
• Continence depends on:
• Stable bladder neck
• Well-supported mid-urethra
• Transmission of intra-abdominal pressure equally to bladder and urethra
The urethra lies:
• Anterior to the vaginal wall
• Inferior to the bladder base
• Embedded in a fibromuscular hammock of fascia and ligaments
Key ligamentous and fascial supports of the urethra
A. Pubourethral ligaments (PUL) – primary continence ligaments
Anatomy
• Paired ligaments extending from:
• Mid-urethra -+ posterior surface of the pubic bone
• Distinct from pubovesical ligaments (see below)
Function
• Anchor the mid-urethra in a fixed position
• Provide a pivot point against which pelvic floor muscles act
Clinical importance
• Integrity of the PUL is essential for stress continence
• Laxity or disruption -➔ urethral hypermobility -+ SUI
• Mid-urethral slings function by replacing or reinforcing the pubourethral ligament
B. Pubovesical ligaments – bladder neck stabilizers
Anatomy
• Extend from:
• Bladder neck and proximal urethra -➔ pubic bone
• Lie superior to the pubourethral ligaments
Function
• Stabilize the bladder neck
• Prevent excessive descent during increases in intra-abdominal pressure
Clinical relevance
• Damage leads to bladder neck descent
• Contributes to mixed or complex incontinence patterns
C. Endopelvic fascia (pubocervical fascia)
Anatomy
• Fibrous connective tissue layer between:
• Anterior vaginal wall
• Urethra and bladder base
• Laterally attached to the arcus tendineus fascia pelvis (ATFP)
Function
• Forms a “hammock” under the urethra
• Transmits pressure forces evenly
• Provides structural integrity for urethral closure during stress
Defects
• Fascial attenuation or tears -+ loss of hammock support
• Central defects -+ urethral descent
• Lateral detachment -+ paravaginal defects
D. Arcus tendineus fascia pelvis (ATFP)
Anatomy
• Dense fascial condensation running from:
• Pubic bone -+ ischial spine
• Serves as the lateral anchoring line for the pubocervical fascia
Function
• Maintains lateral support of bladder base and urethra
• Prevents funneling and rotational descent
E. Uterosacral-cardinal ligament complex (indirect role)
Anatomy
• Suspends the uterus and vaginal apex
• Connects cervix and upper vagina to sacrum and pelvic sidewall
Role in continence
• Provides apical vaginal support
• Apical descent leads to secondary anterior vaginal wall and urethral instability
• Important in post-hysterectomy or advanced prolapse-related incontinence
Functional continence mechanism (integrated model)
- Normal state
• Increased intra-abdominal pressure (cough, laugh):
• Pressure transmitted equally to bladder and urethra
• Urethra is compressed against a firm fascial-ligamentous backboard
• Urethral lumen closes -+ continence maintained
Key contributors
• Pubourethral ligaments (fixation point)
• Pubocervical fascia (hammock)
• Pelvic floor muscles acting through ligamentous anchors
Pathophysiology of stress urinary incontinence Ligamentous failure model (Integral Theory – Petros & Ulmsten)
Primary defect
• Laxity or rupture of the pubourethral ligaments Consequences
• Loss of mid-urethral stability
• Urethra rotates and descends under stress
• Inadequate pressure transmission -+ leakage
- Fascia! failure
- Weak or detached pubocervical fascia
- Urethra lacks a firm backboard
- Leads to hypermobility even if sphincter function is intact
Combined injury
Common after:
• Vaginal childbirth
• Menopause (estrogen-related collagen loss)
• Chronic increased abdominal pressure
• Pelvic surgery
Clinical correlations
Why mid-urethral slings work
• They functionally recreate the pubourethral ligament
• Provide dynamic-not rigid-support
• Restore the normal continence mechanism rather than compressing the urethra
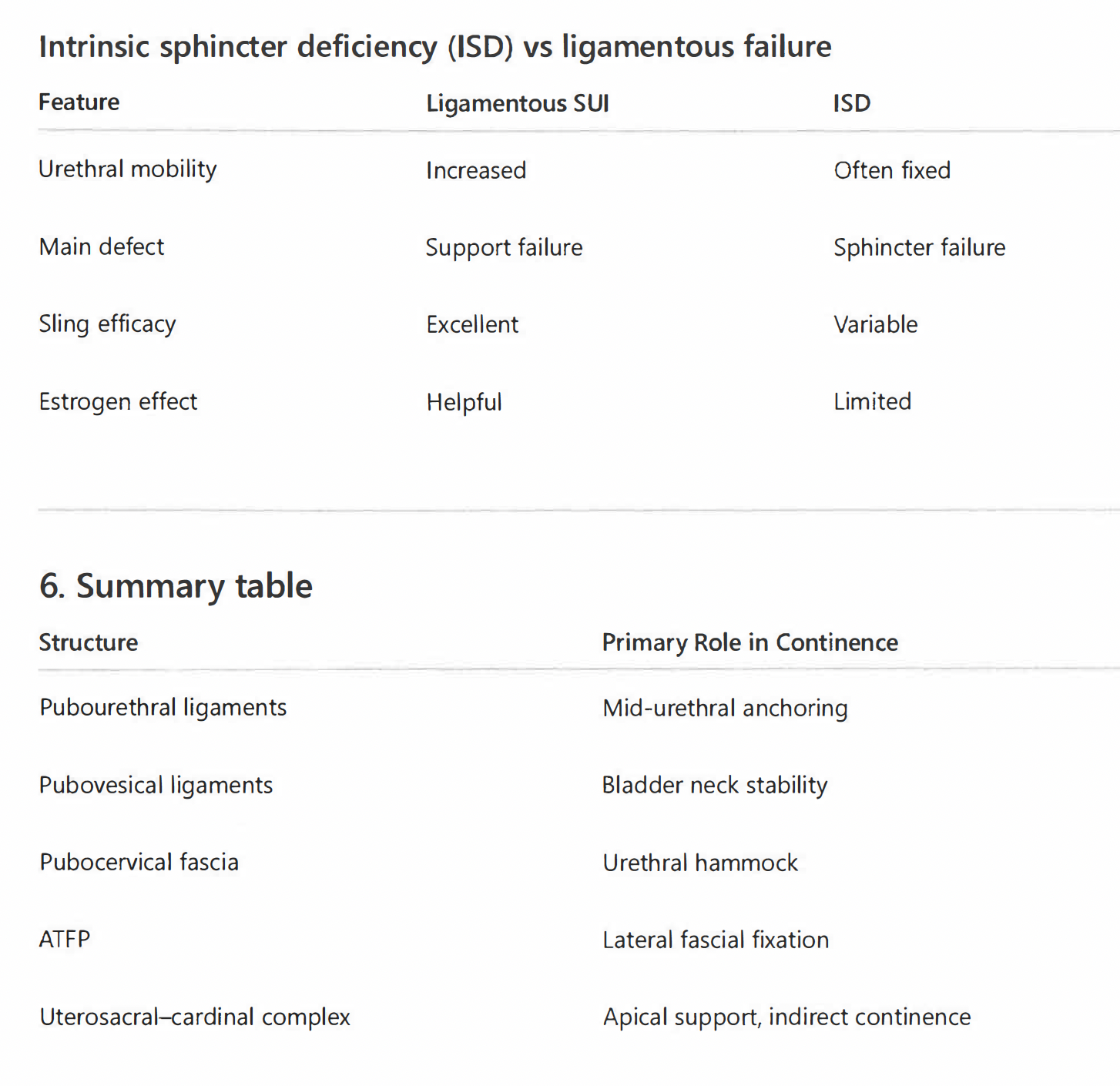
- Intrinsic sphincter deficiency (ISD) vs ligamentous failure
Feature Ligamentous SUI ISO
Urethral mobility Increased Often fixed
Main defect Support failure Sphincter failure
Sling efficacy Excellent Variable
Estrogen effect Helpful Limited
Resources
Notelovitz in 1970, conceptualized a hammock to maintain the normal anatomic position of the female urethra displaced in women with stress urinary incontinence by placing just two sutures on either side of the mid urethra and by tying the proximal and distal threads across the midline created a hammock of tissue that was then suspended to the back of the pubic bone ( see illustrations below).